We have looked at the ability of CRP to predict bacteraemia, which is probably a reasonable proxy measure of sepsis. We looked back at all blood cultures sent to our lab between Jan 2011 and August 2017. This identified 36396 sets of cultures, of which 32703 were negative, 1210 grew a likely contaminant, 1800 grew a likely pathogen and 683 grew an organism isolated in a duplicate set. We then linked this data with concurrent laboratory requests for a CRP. The number of specimens with a CRP measured within 7 days were : 29403 (90%) for negative; 1063 (88%) for contaminant; and 1699 (94%) for an isolated pathogen.
Figure 1 shows the day of the peak CRP measured in the episode. We can see that in episodes with proven infection, there is a lag to peak CRP.

fig.1 Day of peak CRP
We then looked at how the initial CRP predicts bacteraemia. Figure 2 shows the cumulative percentage of episodes in each category at increasing CRP cut-offs (in other words, the number of episodes that would be missed for a particular cut-off CRP value). We can see that 30% of cases of significant bacteraemia have a CRP below 50 on presentation, and over 50% have a CRP below 200.
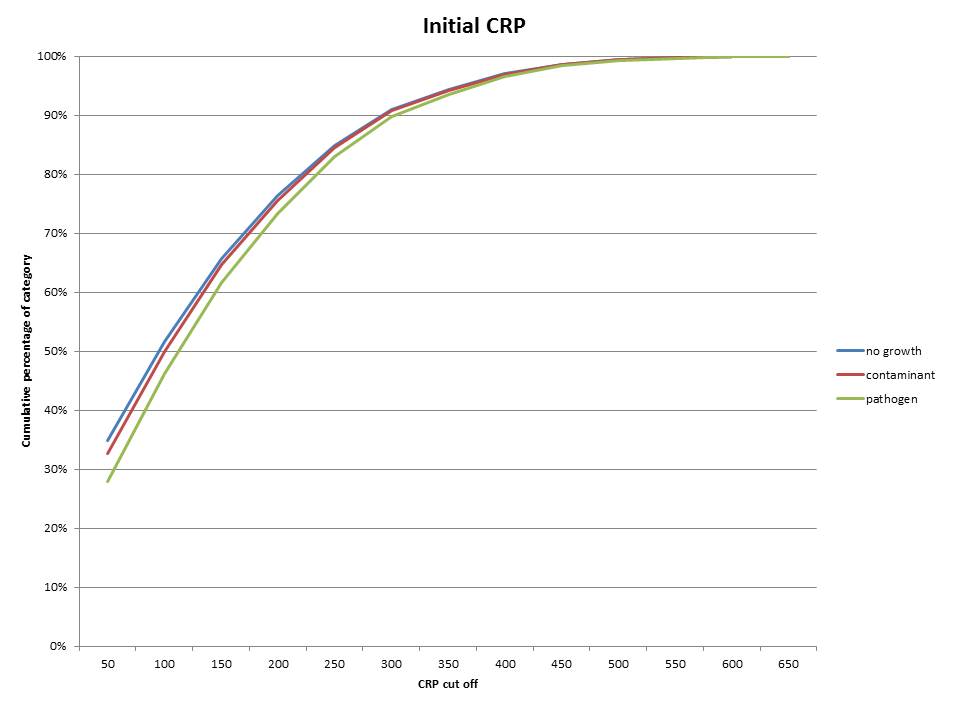
fig 2
The small difference in the curves for the three categories also suggests that initial CRP is not good at discriminating between infection and not infection. We can see this if we plot a receiver-operator curve (fig 3). In a ROC, a test with no value shows a straight line, whereas a good test has a hyperbolic distribution. The initial CRP looks very straight on the ROC. You can draw your own conclusions about the performance of the initial CRP in predicting bacteraemia.

fig 3. ROC for initial CRP in predicting bacteraemia
We then repeated the analysis for the peak CRP measured in the week after the blood culture draw. (fig 4 and 5). So it performs a bit better than the initial CRP, but not a lot.

fig 4

fig 5. fig 3. ROC for peak CRP in predicting bacteraemia
So this is my main conclusion :
It is not possible to find a cut-off value for CRP that tells you anything meaningful about the probability of bacteraemia
We can probably also conclude that there is often a delay between onset of serious infection and rise in CRP. So CRP is really bad at telling us what is going on in an acute setting.
Why are people pushing CRP then? I guess when it was carefully performed in selected cases when it was first brought in as a test, it was quite useful. We can see from our data that there is some signal there, but it's drowned out by noise.
I also suspect that in most cases a CRP is telling us absolutely nothing, but we are using the result to justify our decision making. When it suits us and it confirms our prejudice. Of course, the problems come when there is a mismatch between these two things. People cope with this dissonance in many ways. The most annoying of which is to phone the microbiologist. The most dangerous of which is to make an inaccurate diagnosis.